On April 28, 2017, CMS published the FFY 2018 IPPS Proposed Rule in the Federal Register. After years of discussion on Worksheet S-10 and false starts on the use of uncompensated care data for Medicare DSH/UC pool distribution purposes, CMS appears to have finally moved forward with implementation. Go HERE for our high-level summary of the Medicare DSH/Uncompensated care payment portion of the proposed rule. In this post, we will take a dive into Factor 1 as described in the proposed rule. For a quick refresher on Factor 1, go HERE.
Factor 1 establishes the gross uncompensated care pool. In the FFY 2018 Proposed Rule, CMS continued with a policy established in the FY 2014 IPPS/LTCH PPS final rule of determining Factor 1 by developing estimates of both the aggregate amount of Medicare DSH payments that would be made in the absence of section 1886®(1) of the Act and the aggregate amount of empirically justified Medicare DSH payments to hospitals under 1886®(1) of the Act. In short, CMS estimates the difference between what would have been paid to qualifying hospitals under the historical DSH formula and the 25% empirically justified amount. In determining the DSH estimate for the 2018 proposed rule, CMS used the Office of the Actuary’s January 2017 Medicare DSH projections, which are based on data from the December 2016 update of the Medicare Hospital Cost Report Information System (HCRIS) and the FY 2017 IPPS/LTCH final rule IPPS Impact file, published in conjunction with the publication of the FY 2017 IPPS/LTCH final rule as sources.
Excluded from the DSH estimates are Sole Community Hospitals that are projected to be paid under the hospital-specific rate, Maryland hospitals participating in the Maryland All-Payer Model and hospitals that had been participating in the Rural Community Hospital Demonstration Program.
For FY 2018, the estimate generally begins with cost reporting periods beginning in FFY 2014, with some exceptions. That amount is then trended forward by a number of factors as seen on the table below. CMS applies an annual increase to the DSH estimates, which has worked out to a 6.2% yearly average increase between 2015 and 2018. The proposed 2018 DSH estimate sees a significant increase of 11%. Per the table, the estimate for Medicare DSH payments for FFY 2018 is approximately $16.003 billion versus $14.397 billion in the 2017 final rule estimate. A couple items to note regarding the increase:
Part of the increase is the result of an upward adjustment in the trending factors used in the table below versus the values used in 2017.
Another part of the increase is that the starting point is higher as CMS used FY 2014 cost report data in this proposed rule and used FY 2013 cost report data in the 2017 estimates.
Once the 25% empirically justified DSH is factored in at approximately $4.001 billion dollars, Factor 1 for FFY 2018 is $12,001,915,095.
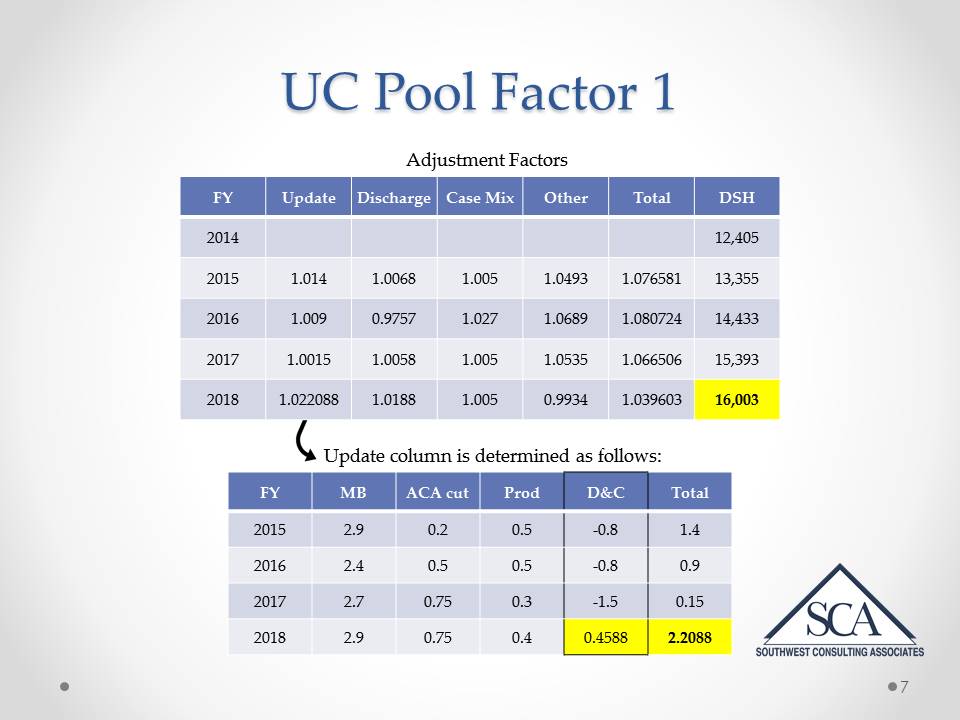
With regard to this table (click image to enlarge), please note the following:
The documentation and coding adjustment used in the Update column, as you can see, is a substantial change from the prior years, particularly compared to 2017. You may recall, the law required the Secretary to recoup approximately $11 billion dollars to account for changes in MS-DRG documentation and coding over a 4-year period beginning in 2014. 2017 was the final year of that recoupment period. However, through subsequent legislation, CMS is required to return those dollars to the hospitals and will be doing so pro-ratably over the period 2018-2023.
The discharge column shows the increase in the number of Medicare fee-for-service (FFS) inpatient hospital discharges. The discharge figures for FYs 2017 and 2018 are assumptions based on recent trends recovering back to the long-term trend and assumptions related to how many beneficiaries will be enrolled in Medicare Advantage (MA) plans.
The case-mix column shows the increase in case-mix for IPPS hospitals. The FY 2017 and 2018 increases are based on the recommendation of the 2010-2011 Medicare Technical Review Panel.
The “Other” column shows the increase in other factors that contribute to the Medicare DSH estimate (difference between total inpatient discharges and the IPPS discharges, various payment rate adjustments and a factor for Medicaid expansion due to the Affordable Care Act). NONE of these components were detailed in the proposed rule.
You will recall from prior years rulemaking notice and comment activities, this component of the “other” adjustment has been controversial. It has been controversial principally based on the fact that CMS has said in the past that utilization among the newly eligible Medicaid recipients is not the same as has been historically experienced because the new enrollees are healthier than the average Medicaid recipient, therefore, fewer hospital services are consumed. The result on the calculation is that the “full” value of projected DSH associated with expansion is not included in the Factor 1 calculation – however, the “full” value of those people are counted in the number of insured in Factor 2, which does reduce the amount of the UC pool.
This is certainly an area that hospitals will want to examine and determine if further comment is warranted as even though CMS did not show the math on this adjustment, the expected result is that the 2018 DSH number is not as high as it might otherwise be, since CMS has made this limiting assumption regarding Medicaid expansion and what services are being utilized by the newly expanded population.
That wraps up a detailed look at Factor 1 from the FY 2018 proposed rule. Remember public comments will be accepted until 5 p.m. EDT on June 13, 2017. If finalized, these changes will go into effect October 1, 2017.
Up next, an in depth look at Factor 2. Stay tuned.
Don't miss the subsequent blog posts in our FY 2018 IPPS Proposed Rule series and SUBSCRIBE TO OUR BLOG BELOW!
